ABO incompatibility is one of the diseases which can cause jaundice. It happens when a mother's blood type is O, and her baby's blood type is A or B.
Jaundice In Babies
Jaundice In Babies
Mild jaundice is common in pēpi (babies), but baby jaundice is not always normal. If your baby has yellow skin or eyes and pale poo or dark (yellow or brown) wee, your baby needs a special blood test. See a health professional or midwife as soon as possible.
Key points about jaundice in babies
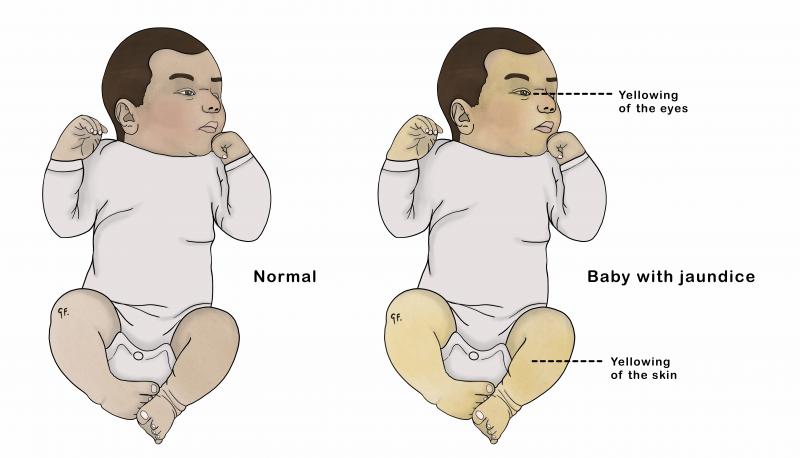
- jaundice means yellow colouring of the skin and the whites of the eyes
- mild jaundice is common in newborn pēpi - it starts on the second or third day and settles over 7 to 10 days
- there are many causes of jaundice
- some types of jaundice are serious
- jaundice that appears in the first 24 hours after birth is not normal - it needs checking by a health professional straight away
- jaundice at any age with pale poos and dark wee needs checking with a blood test
- jaundice still there after 2 weeks of age needs checking by a health professional
- every month, a New Zealand baby is born with severe liver disease which can show as jaundice
- severe jaundice can be serious - with correct early treatment, long-term problems are rare
What is jaundice?
Jaundice is the medical word for the yellowing of the skin and the whites of the eyes.
What causes jaundice?
Jaundice is caused by a substance in the blood called bilirubin. At low or medium levels, jaundice does not cause problems. At high levels, bilirubin can be harmful. It can lead to deafness or brain damage. Pēpi with high levels need immediate treatment.
Are there different types of jaundice?
Jaundice is very common - over half of all pēpi have it. There are different reasons why a pēpi may have jaundice.
Physiological jaundice
In most pēpi, jaundice is normal and natural and settles as the baby's organs mature and adjust after birth. The medical term for this type of jaundice in newborns is physiological jaundice. This type of jaundice does not usually harm pēpi.
Breastmilk jaundice
Some breastfed pēpi may stay jaundiced for longer than formula-fed pēpi. This is because of a normal and natural effect of breastmilk on pēpi. This type of jaundice is called breastmilk jaundice. It is not harmful and breastfeeding should continue.
Liver problems
There are many other reasons for jaundice, and if you are concerned, you should talk to your midwife or health professional. Each year in New Zealand, a small number of pēpi are born with liver disease, which also causes jaundice. This is not normal and a health professional or midwife needs to see this.
Other conditions
Jaundice can occur in pēpi with other conditions such as inherited conditions or when there are problems with their blood type. This includes conditions such as:
How do I know if my baby's jaundice is normal?
Jaundice is likely to be normal if your baby:
- becomes jaundiced after the first 24 hours after birth
- wakes themself up to demand feeds
- looks well and feeds well
- has yellow or green poo (not pale, white or light beige poo)
- has wee, which is clear or straw-coloured, not yellow or dark
As the bilirubin level gets higher, your baby:
- will become more obviously yellow over the whole body
- may be sleepy and slow to wake up for feeding
- may feed less well
If you are worried or have questions, ask your midwife or health professional to check your baby.
How long will my baby's jaundice last?
Normal (physiological) jaundice usually fades away after 1 or 2 weeks. Sometimes, normal jaundice may last longer than this.
When should I seek help for my baby's jaundice?
You should seek help if any of the following situations apply to your baby.
If your baby is jaundiced in the first 24 hours after birth
Jaundice in the first 24 hours after birth is never normal and needs urgent medical attention. Contact your midwife or a health professional straightaway.
If your baby is still jaundiced at 2 weeks of age
If your baby is still jaundiced 2 weeks after birth, your health professional or midwife will need to check them. Your baby will need a blood test and may need to see a paediatrician - a doctor specialising in pēpi and tamariki (children).
It is important not to miss any of the rare causes of jaundice that need special treatments. Biliary atresia is one of these important conditions.
See the KidsHealth page on biliary atresia for more information.
If your baby is jaundiced and has pale poos or dark wee
If your baby is jaundiced and has pale, white or light beige-coloured poo, take them to a health professional. The health professional can arrange an urgent appointment with a paediatrician.
The photo below shows a nappy with pale poo and dark wee.

If your baby is jaundiced and unwell
You should call your midwife or a health professional urgently if your baby is jaundiced and:
- looks sick
- is jittery (trembling)
- has an unusual cry
- is becoming more obviously yellow over their whole body
- is sleepy and slow to wake up for feeds
- is feeding poorly
- is getting dehydrated (dry) - signs include not having wet nappies
You should also talk to your midwife or a health professional if your baby:
- has not passed meconium (the first black bowel motion) by the second day
- is at increased risk of severe jaundice
What puts my baby at risk of getting severe jaundice?
There are a number of conditions that increase the chance of your baby getting jaundiced.
Blood type incompatibilities
ABO incompatibility is one of the diseases which can cause jaundice. It happens when a mother's blood type is O, and her baby's blood type is A or B.
See the KidsHealth page on ABO incompatibility for more information.
Rhesus disease can cause jaundice. It can only happen if a mother's blood type is Rhesus negative and her baby's blood type is Rhesus positive.
See the KidsHealth page on rhesus disease for more information.
Inherited conditions
Some inherited conditions, such as hereditary spherocytosis and G6PD deficiency, can cause jaundice. G6PD deficiency can cause jaundice at any age, including in newborn pēpi.
See the KidsHealth page on G6PD deficiency for more information.
Prematurity
Pēpi who are born early have an increased chance of developing jaundice because their liver is premature as well.
Infections
Infection that begins before or after birth can increase the chance of a baby having jaundice.
Other conditions
Other more uncommon medical conditions like cystic fibrosis and thyroid disorders can cause jaundice.
How is jaundice diagnosed?
If your baby's skin is yellow, and the white parts of their eyes are yellow, then your baby is jaundiced. In most newborn pēpi, jaundice is normal and natural.
A blood test gives more information about the level of jaundice.
The health professional will arrange a blood test if:
- the jaundice appears before 24 hours of age
- your baby appears very yellow
- the jaundice lasts more than 2 weeks
- your baby has pale poo or dark wee
- there are other concerns
What treatments are available for jaundice?
If your baby has normal (physiological) jaundice, they will not need any special treatment. You can treat mild jaundice in the first week by simply making sure that your baby has enough fluid, and you do this by breastfeeding. Breastfeeding gives your baby essential food and the right amount of water. Pēpi do not normally need extra water. Regular feeding to boost the supply of breastmilk is important.
Phototherapy
If the bilirubin level is high, phototherapy (bright light therapy) is the most commonly used treatment. It does not contain rays that would harm your baby. Phototherapy is very safe and effective and can only happen in hospitals.
See the KidsHealth page on phototherapy for more information.
Extra tests
A small number of pēpi with severe jaundice may have liver disease. Your baby may need blood tests or to go to hospital to see a specialist doctor for tests, especially if the jaundice does not go away by 2 weeks of age or your baby has pale poo or dark wee.
Are there likely to be any complications from jaundice?
When pēpi receive the correct treatment, complications of jaundice are rare. Severe jaundice can lead to deafness or brain damage without diagnosis and quick treatment.
Points to remember about jaundice in newborn pēpi are:
- there are many causes of jaundice
- some types of jaundice are serious
- jaundice that appears in the first 24 hours after birth is not normal - it needs checking by a health professional straight away
- jaundice at any age with pale poo and dark wee needs checking with a blood test immediately
- jaundice still there after 2 weeks of age needs checking by a health professional
- severe jaundice can be serious - with correct early treatment, long-term problems are rare
See the 'Beware yellow' poster (PDF, 259KB) for symptoms to be aware of in jaundiced babies.
The poster is also available in:
This page last reviewed 20 March 2024.
Do you have any feedback for KidsHealth?
If you have any feedback about the KidsHealth website, or have a suggestion for new content, please get in touch with us.
Email us now