
Key points about supraventricular tachycardia (SVT)
- an abnormally fast heart rhythm is called tachycardia
- tachycardias can start in the upper or lower chambers of the heart
- tachycardias that involve the upper chambers are called supraventricular tachycardia or SVT
- SVT is usually not dangerous
- SVT is not due to a 'heart attack'
- in tamariki with an otherwise healthy heart, SVT does not cause sudden death
What is supraventricular tachycardia (SVT)?
The heart beats because of electrical signals that travel through it in a set pattern. Health professionals can see the heart's electrical activity by using an electrocardiograph (ECG).
An abnormally fast heart rhythm is called tachycardia. This can start in:
- the lower chambers of the heart (the ventricles), or
- the upper chambers of the heart (the atria)
Tachycardia that starts in the lower chambers is called ventricular tachycardia.
Tachycardia that involves the upper chambers is called supraventricular tachycardia (SVT).
SVT is usually not dangerous. It is not caused by a heart attack. In tamariki with an otherwise healthy heart, SVT does not cause sudden death.
But, if SVT happens very often or lasts a long time (hours to days), it can affect how well the heart pumps blood. This can become serious if it is not treated.
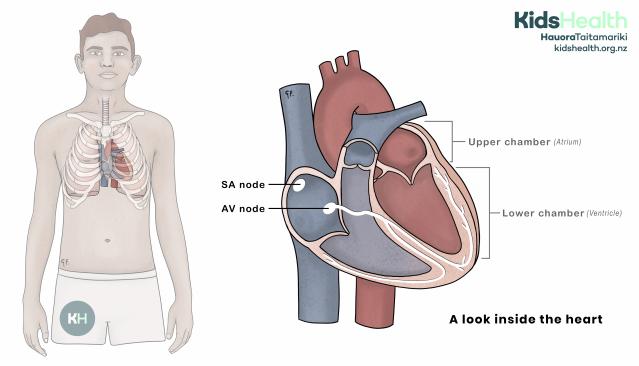
This illustration shows the heart’s location in the chest and a close-up view of its chambers and the SA and AV node. Electrical activity moves from the SA node to the AV node and down through the fibres illustrated in white.
Source: KidsHealth
transcribeTranscript
On the left, the illustration shows a teenage male. The ribcage is visible, with the heart shown inside the chest between the lungs.
On the right, there is an enlarged cross-section of the heart. The heart has two upper chambers (atria) and two lower chambers (ventricles). Two small white circles inside the right atrium are labelled SA node and AV node. Thin white lines run through the heart muscle, showing the heart’s electrical conduction pathways.
The text beneath reads: ‘A look inside the heart.’
At the top right is the KidsHealth logo with the website: kidshealth.org.nz
How electrical signals normally move through the heart
The electrical signal starts in the SA node. The SA node is the heart's own natural pacemaker.
The electrical signal moves to the AV node. The AV node sits between the upper and lower chambers of the heart.
The electrical signal moves down through the lower chambers of the heart.
This organised flow of electrical activity keeps the heart beating at a steady, regular pace.
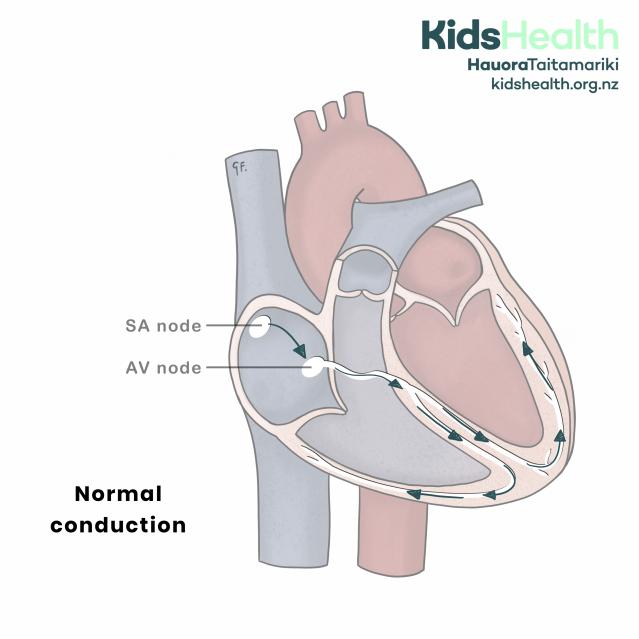
Normal conduction of electrical signals through the heart.
Source: KidsHealth
transcribeTranscript
The illustration shows a simplified cross-section of the heart. The right atrium contains the SA node (sinoatrial node) at the top and the AV node (atrioventricular node) lower down. Curved arrows show the pathway of electrical activity through the heart:
- Starting at the SA node in the right atrium
- Moving to the AV node
- Travelling down into the ventricles and spreading through both lower chambers via the branches (shown in white).
The text at the lower left reads: ‘Normal conduction’.
At the top right is the KidsHealth logo with the website: kidshealth.org.nz
Types of SVT
Atrial tachycardia
In atrial tachycardia, a small area in the upper chambers takes over the pacemaker role of the heart. This type of SVT is uncommon in tamariki.
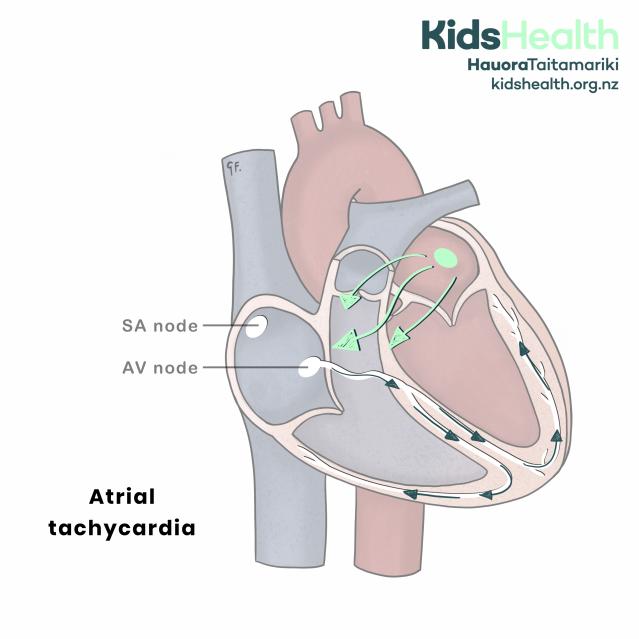
Atrial tachycardia.
Source: KidsHealth
transcribeTranscript
The illustration shows a simplified cross-section of the heart. The right atrium contains the SA node at the top and the AV node lower down. In this diagram, a green dot and arrows in the upper right atrium show an abnormal starting point for the electrical impulses, instead of starting at the SA node.
Green arrows trace the abnormal signals from the atrium to the AV node, and dark blue arrows continue from the AV node into the ventricles, spreading through both lower chambers.
The text at the lower left reads: ‘Atrial tachycardia’.
At the top right is the KidsHealth logo with the website: kidshealth.org.nz
Atrial Flutter
In atrial flutter, a large area of the upper chamber forms a fast electrical loop.
This rhythm is more common in tamariki who have had heart surgery on the upper chambers before. Some tamariki with atrial flutter are at risk of developing blood clots. This is because blood flow in these chambers can be slow and disorganised.
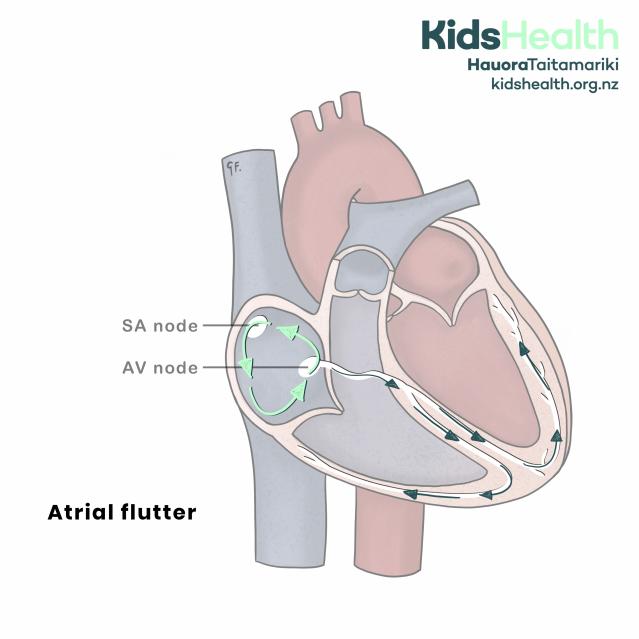
Atrial Flutter.
Source: KidsHealth
transcribeTranscript
The illustration shows a simplified cross-section of the heart. The right atrium contains the SA node at the top and the AV node lower down. In this diagram, green arrows show a continuous loop of abnormal electrical signals circling inside the right atrium.
The text at the lower left reads: ‘Atrial flutter’.
At the top right is the KidsHealth logo with the website: kidshealth.org.nz
Atrio-ventricular re-entrant tachycardia (AVRT)
In AVRT, there’s an extra electrical link between the heart’s upper and lower chambers. This extra pathway is called an accessory pathway. It lets the electrical signal loop around instead of going in one direction. This causes a very fast heart rate.
This is the most common type of SVT in tamariki under 8 years of age.
Many pēpi (babies) with this type of SVT grow out of it during their first year of life. In some tamariki, it can return later in childhood.
Some specific conditions in this group include:
- Wolff–Parkinson–White (WPW) syndrome
- Permanent junctional reciprocating tachycardia (PJRT)
In older tamariki, WPW can rarely be life-threatening. Your child’s doctor may recommend special tests and a treatment called ablation. This is a keyhole procedure where the heart is reached through the veins at the top of the leg.
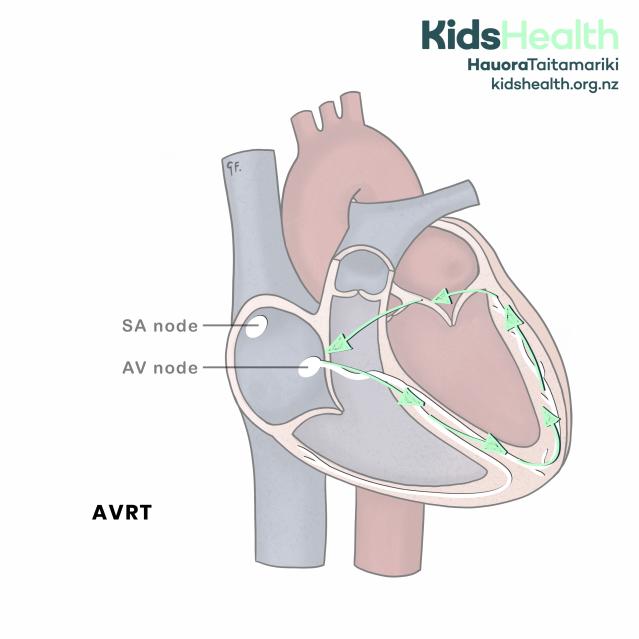
Atrio-ventricular re-entrant tachycardia (AVRT).
Source: KidsHealth
transcribeTranscript
The illustration shows a simplified cross-section of the heart. The right atrium contains the SA node at the top and the AV node lower down. Green arrows trace the abnormal pathway:
- The signal travels from the SA node to the AV node,
- Down into the ventricles,
- Then back up into the atria through an extra pathway, creating a reentrant loop.
This looping pathway repeats rapidly, causing the heart to beat faster.
The text at the lower left reads: ‘AVRT’.
At the top right is the KidsHealth logo with the website: kidshealth.org.nz
Atrio-ventricular nodal re-entrant tachycardia (AVNRT)
The AV node normally controls how electrical signals pass through the heart. Electrical signals usually pass from the upper to the lower chambers of the heart. Sometimes the AV node can cause a fast rhythm itself.
This is the most common type of SVT in tamariki over 8 years of age.

Atrio-ventricular nodal re-entrant tachycardia (AVNRT).
Source: KidsHealth
transcribeTranscript
The illustration shows a simplified cross-section of the heart. The right atrium contains the SA node at the top and the AV node lower down. Green arrows form a small loop around the AV node, showing the abnormal pathway of the electrical signals.
From the loop, impulses travel into the ventricles, shown by dark blue arrows, and spread through both lower chambers. This looping pathway inside and around the AV node repeats rapidly, causing a fast heartbeat.
The text at the lower left reads: ‘AVNRT’.
At the top right is the KidsHealth logo with the website: kidshealth.org.nz
How to recognise if your child has SVT
Recognising SVT in children and young people
Older tamariki and rangatahi with SVT may notice:
- a sudden fast heart rate (palpitations)
- their heart racing at unexpected times - such as while resting, after exercise, or after eating
Younger tamariki may find it hard to describe what they feel. They may complain of chest pain or seem unsettled.
SVT can rarely cause tamariki or rangatahi to pass out.
Recognising SVT in babies
Some pēpi can become unwell if SVT has been happening for a long time, including before birth. In most infants, SVT is well tolerated if it is picked up within a few hours of starting.
You might notice a fast heart rate while feeding or cuddling your baby. If SVT continues, some infants may develop:
- poor feeding
- irritability
- pale skin
- fast breathing
If your baby has frequent fast heart rates or shows these signs, see a health professional.
When to get urgent medical help for your child
During a bad episode of SVT, your child may:
- feel dizzy or drowsy
- look pale, cold, or sweaty
- pass out
Learning how to take your child’s pulse can help you recognise when their heart rate is too fast.
Call 111 and ask for urgent medical help if you child:
- becomes very unwell
- passes out during an attack
If the cause is SVT, your child usually wakes quickly once they are lying flat. Keep your child lying down or sitting until they fully recover. You can try vagal manoeuvres (see below) with your child.
Preventing SVT attacks
Some tamariki take medicines every day to help prevent SVT attacks. The medicine chosen depends on the type of SVT.
Common medicines include:
- Sotalol
- Flecainide
- Atenolol or Propranolol
- Amiodarone
Managing SVT attacks
Vagal manoeuvres
Vagal manoeuvres can sometimes stop an SVT episode by slowing the heart. These work by stimulating the vagus nerve causing the heart to slow.
Babies
For pēpi - place a cold (iced) flannel over the eyes for about 10 seconds. In hospital only, doctors may briefly place a baby’s face in cold water for a couple of seconds.
Children and young people
For older tamariki - ask them to try blowing hard with their thumb in their mouth. A very cold drink or standing on their head may also help.
Medicine
In hospital, health professionals can give medicine into a vein to stop SVT. Common medicines include Adenosine and Amiodarone.
Electrical cardioversion
Electrical cardioversion is rarely needed. This is rarely needed. It involves giving a controlled electrical shock to reset the heart rhythm. It happens while your child is under a short general anaesthetic.
Can SVT be cured?
If SVT continues into school age, your child may need another type of treatment. Radio-frequency ablation is a procedure that can cure SVT. Radio-frequency ablation involves a heart catheter study. Special wires are passed to the heart through veins at the top of the leg. Doctors map the heart’s electrical pathways and disable the area causing the problem. The procedure is usually done while your child is asleep under a general anaesthetic.
Acknowledgements
Illustrations by Dr Greta File. Properly of KidsHealth.